

2014
2014 DSN AGM & Conference
Saturday 11th October 2014
at the Human Rights Action Centre in London
Programme
10.00 AGM & Election of Committee
11.30 The GMC – Who Watches the Watchers?
Dr Clare Gerada, MBE, FRCP, FRCGP, MRCPsych, Director, Practitioner Health Programme
12.30 Occupational Health: how we can help
Dr Janet Ballard, Consultant Occupational Health Physician, West London Mental Health Trust

Human Rights Action Centre
14.30 Experiencing and Exploring Mindfulness
Dr Elwyn Perry, Mindfulness Practitioner
15.00 Cracking up, Cracking on
Bobby Baker, Artist
16.15 Clowning and Self-Compassion
Dr David Wheeler, General Practitioner
Sponsored by

-

Dr Clare Gerada
-

Dr Janet Ballard
-

Dr Elwyn Perry
-

Bobby Baker
-

Dr David Wheeler





2014 BMJ Careers fair

DSN has run a stand at the annual BMJ Careers fair for the last few years. This is a good event for DSN with many attendees including doctors and employers. We use this event to 'get the word out' about DSN - that we exist!
2014 International Conference on Physician Health
September 2014 at BMA House
DSN attended the International Conference on Physician Health
in London en masse! ICPH is a collaboration between the American Medical Association, the Canadian Medical Association and the British Medical Association and is held every other year with the venue rotating around the three associations.

DSN sponsored a stand and spoke to many interested delegates from around the world. Several attendees were particularly interested in how DSN works as they are considering setting up a similar support network at home.
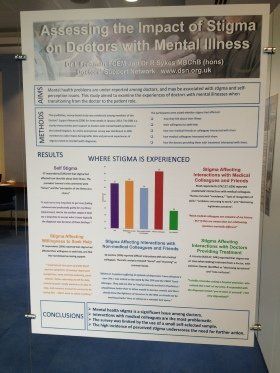
The DSN stigma survey
poster was published at the conference. DSN member Mhairi Hepburn also had a poster at ICPH about a support website for medical students with mental health problems. Another DSN related poster was presented by Michael Ridley-Dash on his research study of DSN GP members.

Reflections on ICPH 2014
Dr Alison Holt
Fifteen years ago I believed that doctors could not get ill, that I could not be ill. I was forcefully disabused of this notion. But when recovered I had to go back into the world where unwell doctors were an anathema, if they were acknowledged at all. In the intervening years I have become involved in supporting others, through DSN and elsewhere, and a lot of what I do is awareness raising- popping up at conferences and training events to make the case that doctors get ill and that getting help is difficult. And audiences range from hostile, through dismissive, to accepting and interested. But always is the need to explain, to justify what I am saying, to "make a case".
The most enjoyable thing for me about the International Conference on Physician Health was spending three days surrounded by people who already 'get it' – who understand that there is a problem and are actively involved in trying to solve it – be that through policy, education, service provision or research.
Refreshing, re-energising, inspiring, interesting and affirming. Not often you can say that after three days of study leave!
Dr Louise Freeman
I was interested that there were frequent references at ICPH to the needs of sick doctors for advocates. We recently heard at the DSN conference that occupational health practitioners cannot be advocates due to their responsibilities towards doctors and employers. So who should be the advocate for the sick doctor? Doctors providing specialist services to sick doctors would seem to be the obvious candidates for this role. I wondered if physician health practice in North America differs from that in the UK given that the Canadian and US doctors seemed very comfortable with this concept.
Sarah
It was a real privilege to attend the ICPH and help to man the DSN stand. As a relatively new member of DSN, it was lovely to meet people face-to-face and to support each other in person. While manning the DSN stand, we met people from all over the world, explaining the set-up of DSN and sharing experiences. Support networks for doctors have been set up in many countries, but often with a “top-down” structure, rather than providing peer support (like DSN does). It was also a privilege to be able to attend the plenary sessions and seminars throughout the conference.
Is a Career in Medicine Suitable for Women?
A highlight for me was attending a talk given by Dr Clare Gerada, entitled, “Is a career in medicine suitable for women?” The talk was structured around data from the Practitioner Health Programme (PHP)1.
Over the past five years, PHP has seen a surge in young doctors (aged 25–35 years) consulting the service; the majority of whom are women, with a peak age of 29–30 years. Several postulations were given for this:
1. Characteristics of “good doctors” (e.g. perfectionism and altruism) make us more vulnerable to mental health problems.
2. The NHS is a toxic, barbaric environment within which to work, with a culture of bullying and blame.
3. As a trainee, there is very little stability: we cannot guarantee where we will work, what our next placement will be, and where we will live. The lack of a “firm structure” at work also means that we may be working with different people each week, leading to further instability.
4. Young female doctors look around at their peers - many of whom by the age of 28–30 years have a stable career, a partner, and children. It is hard to ignore the “biological clock” ticking away … this creates tension between progressing through training and wanting to settle down to start a family.
5. We are exhausted from working erratic shift patterns, which disrupt continuity, reduces resilience and causes exhaustion.
The good news is that once women access the service provided by PHP, they do remarkably well. The majority are back to full functioning after five or six sessions of cognitive behavioural therapy and have an increased awareness of how to avoid a relapse. But fundamentally, the working environment needs to be reviewed to make it less “toxic”; to provide more continuity and stability (e.g. by restoring firm structure); which, in turn, will lead to increased resilience and reduce disruption to everyday life.
Reference:
1. Gerada C, Jones R, Wessely A. Young female doctors, mental health, and the NHS working environment. BMJ Careers 9 Jan 2014.
-

DSN Stigma survey 2014 poster
-

GP psych distress poster

2014 UK Association for Physician Health annual meeting
June 2014
at BMA House
The United Kingdom Association for Physician Health (UKAPH) was founded in 2012 and is chaired by Dr Mike Peters of the BMA Doctors for Doctors unit. The aim is to bring together professionals from a variety of backgrounds including psychology, occupational health, psychiatry, and general practice - with a common aim to improve the mental health of UK doctors.
By Dr Louise Freeman
Novel ways of supporting unwell doctors
The programme opened with a presentation from Dr Clare Gerada (medical director of the Practitioner Health Programme) and Debbie Cohen (occupational physician) on the subject of ‘Supporting doctors away from the workplace’. Clare referred to barriers to getting doctors back to work, such as general practitioners being required to sit an MCQ and viva before being allowed to practise. She suggested that this made it much more difficult for older doctors to return to work in this speciality. Debbie listed a variety of obstacles to doctors seeking help with mental ill health including lack of knowledge from employing organisations. Then, Dr Sally Coomber (consultant occupational physician with Public Health England) introduced her suggested pathway for managing unwell healthcare professionals. There was much discussion during a group work session on this topic.
Effect of complaints on doctors
The most controversial session of the day was ‘The effect of complaints on doctors’ presented by Anna Rowland (assistant director of policy at the GMC) and Dr Michael Peters (medical director of BMA Doctors for Doctors). During this session, a recent survey by the GMC of suicides among doctors who had undergone the fitness to practice process was referred to, as was a survey by the BMA on the impact of complaints on doctors – both surveys are unpublished. The conclusions from both pieces of work implied that the process through which fitness to practice complaints were handled could be improved to avoid unintended negative consequences for the individual involved. But, the most animated discussion was around whether individual doctors undergoing fitness to practice had underlying factors which had predisposed them to suffering from related ill health.
Blaming the individual
Having reflected, I personally feel that blaming the individual is common to many stigmatising conditions. When an individual is affected, it is common to look for predisposing factors, even where the underlying incidence of the condition is known to be high in a population. For example, doctors are known to be at higher risk of stress, and this effectively blames the individual for their illness.
Finally, Abigail Moore (BMA industrial relations officer) discussed how to support doctors experiencing bullying and harassment. The day concluded with a group work session where all present contributed to how to take UKAPH forwards, with developments such as a website on which good practice from one area could be publicised to help other regions, thereby reducing the ‘silo working’ referred to by Clare Gerada.
NHS Practitioner Health Programme 'Five years on'
14th May 2014
10.00 Introduction:
Dr Clare Gerada – Medical Director of the NHS Practitioner Health Programme
Prof. David Walker – Deputy Chief Medical Officer, DH England
The Patient’s Story: PHP patients share their experiences
The Clinician’s Experience:
Richard Jones, Specialist Nurse, PHP
A Commissioner’s perspective: The Impact of the NHS PHP
:
Louisa Dallmeyer, Specialist Commissioning, Office of London CCGs
Future Challenges: round-table discussions
13.15 Workshop
- “Treating the Addicted Doctor” –
Dr Jane Marshall, PHP
- “Working with Occupational Health for Practitioner Health” – Dr James Anderson, PHP & Dr Janet Ballard
- “Health and Performance”
– Richard Jones, PHP Clinical Director
The importance of identifying health needs and providing support to doctors:
Prof Terence Stephenson
16.00
Closing comments:
Lucy Warner, Chief Executive, PHP
2014 London Marathon
April 2014
Dr. Oliver Quantick raised £1100 for DSN by running the London Marathon!
Find out more about raising money for DSN here.
Destigmatising Healthcare for Healthcare Professionals
By Dr Louise Freeman
February 2014
The Doctors’ Support Network was pleased to be invited to contribute to a ‘De-stigmatising Healthcare for Healthcare Professionals’ day run by the Professional Support Unit of the London Deanery. The event was aimed at doctors and managers involved in helping sick staff. Angelika and I manned the (free) DSN stand during which we spoke to a mixture of doctors, human resources (HR) staff and others about DSN.
The programme started with a key note lecture from Dr Steve Boorman, consultant in occupational medicine. His name may be familiar from his role as the lead for the NHS Health and Wellbeing review in 2009. Dr Boorman illustrated his talk with a short, anonymous case history of a consultant who had acquired an alcohol problem after a series of devastating personal events. This led to problems at work and the doctor was suspended. The doctor saw a General Practitioner (GP) as a temporary resident. The GP’s response was “what do you want me to do about it?”. The doctor then detoxed from alcohol on their own during the course of which they were admitted to a psychiatric unit and discharged with no follow-up after which, the doctor’s employer used the disciplinary process to terminate their contract. It was interesting to me that Dr Boorman was obviously angry that this sub standard process had taken place.
Various workshops followed including ‘The Role of Insight in Physician Performance and Remediation’
delivered by Dr Nick Brown, a consultant psychiatrist who is also a senior assessment advisor with the National Clinical Assessment Service (NCAS). Dr Brown discussed how insight is not a fixed quality but can change over time. He stressed the important points that there is no single tool for assessing insight and it should also be evaluated independently of other clinical assessment processes. We then did a practical exercise in which Dr Brown showed us relationship maps from sample cases in which the index doctor maps their personal and professional interactions with others by drawing a series of circles with the size of the circle corresponding to the importance of the individual in the relationship. The doctor then draws uni or bi directional arrows to show how interactions work between the individuals. We discussed the sample maps in small groups and drew conclusions as to what the maps meant for the individual doctors. Finally, Dr Brown made the interesting point that in 10% of the cases taken forwards by NCAS, the referring employer admits that there might be an organisational issue. In contrast, NCAS finds that 80% of cases have an underlying organisational problem. He stressed that NCAS can only recommend actions and is not a regulator.
In the afternoon, Angelika learnt about ‘Managing the older worker’ from which her conclusions were that there is no evidence of cognitive decline as a natural ageing process. I attended ‘Sad, mad or bad, or the result of the system? Tackling grey area problems in physician mental health’
facilitated by Dr John Launer. This was an interesting session in which participants spoke about complex staff management cases in which they had been involved and we were encouraged to contribute. The most interesting aspect for me was hearing how HR professionals can sometimes rush into formal processes to manage ill health when informal may be more effective at that stage. I understood the HR point of view much better post workshop – they are often criticised for not using processes soon enough!
The last session of the day was a panel discussion in which I represented DSN on an expert panel. Unfortunately there was insufficient time to allow the discussion to develop but DSN very much support service user involvement in this type of event. Overall, the day was excellent and there are obviously many great programmes in place around the UK. But this was very much preaching to the converted and I will give the final word to Dr Chris Manning who said that he had been attending these events for 15-20 years and hearing similar well -meaning addresses. “Why don’t we just do it?”
